Immunologist Ravindra Gupta teaches clinical microbiology at Cambridge University. He has been researching Covid-19 variants and advising the British authorities on containing their spread. Speaking to Srijana Mitra Das at Times Evoke, Gupta discusses his insights:
What does the scientific community know about Covid-19 variants?
The consensus is firstly, these variants emerged in individuals who had a longterm infection. It’s the only plausible way by which you can see so many variations of the virus arising in a short span of time. We’ve presented definitive research on this in the journal Nature earlier this year. Other viruses don’t do this — Covid-19 is an unprecedented virus because it can infect people for weeks and months and during that time, it can learn to adapt and make mutations that enable it to gain advantage. When the virus then transmits to other people, it has this added power of mutations that enable it to be optimised in a very short period of time.
However, what we also know is that the Covid-19 vaccines protect against severe illness and loss of life, even with variants which show some immune-escape mutations, as seen in the South African and Brazilian variants and, to some extent, the B.1.617 Indian variant.
Why does the Indian variant seem so much stronger?
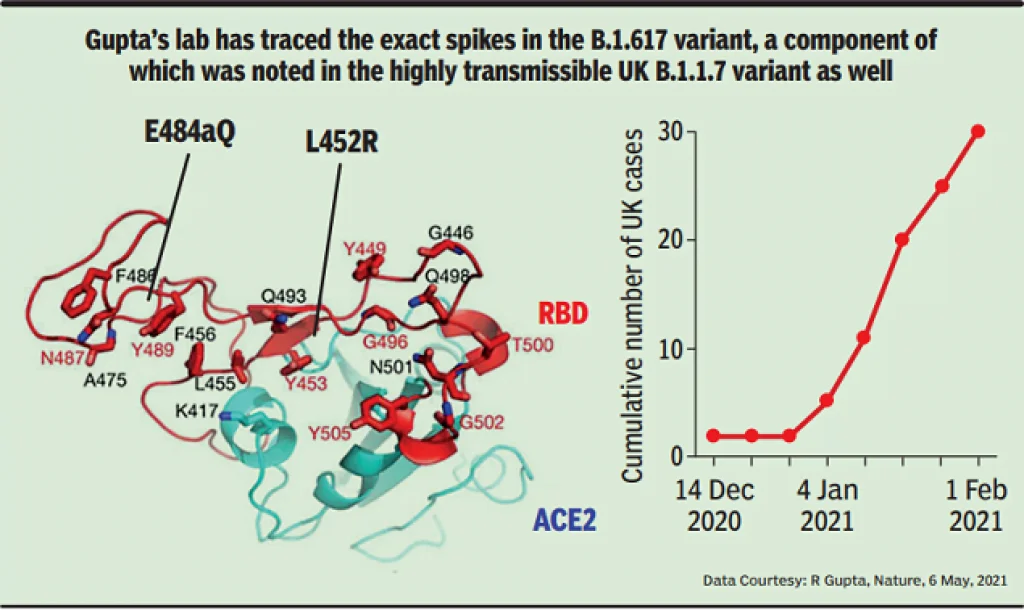
The ‘double mutant’ term for this was coined by scientists who saw a virus with two mutations in the key part of the protein that engages our cells and threatens our antibodies. The two mutations are at spike positions 452 and 484 (see diagram) — they’ve never been seen together in a highly transmissible virus.
One of the mutations L452R is in the California variant which spread earlier in southwestern America and was considered more transmissible than the original strain. The other mutation at position E484 is much less known — but our research shows that the amino acid glutamine symbolised by ‘Q’ does not have such a dramatic impact as the ‘K’ or lysine in terms of avoiding antibodies. People initially saw them together and assumed this was a double mutation which would have a serious impact on vaccine efficacy, based on the assumption that their effects would add up. However, our research shows that this is not the case.
This form of the virus has some loss of the neutralisation capability of antibodies from people who are vaccinated — it’s around five-fold which is not a huge amount but it can be appreciable in people whose immunity is not as strong as others. That could explain why we are seeing people being infected, despite the vaccine, or being re-infected. This mutation has developed some capacity to get around people’s antibodies — but this is not as massive an effect as predicted earlier.
Do viruses weaken over time?
Viruses do become more benign but over long periods of time. In the immediate timeframe, the virus tries to survive in a hostile environment, which is our immune system. It gains mutations that enable it to become stronger than its competitors by trying to survive within people who have chronic infection — people who were infected six to eight months ago could have their antibodies dropping by now. As immunity declines, infections start to rise. And with the new variants, we’re also seeing far greater infectiousness and more transmission capability.

How do vaccines combat this?
With a vaccine, we show our immune system an example of the virus ahead of time, so that if a person gets infected with the real thing, the immune system can completely destroy it. A good scientific strategy would be to thoroughly understand variants and engineer yearly vaccines to fight these. This requires considerable investment but we’ve done it earlier for influenza, so this should not be more difficult.
Apart from vaccines, social distancing is crucial — in the UK, we stopped the B.1.1.7 variant with three months of lockdown. These viruses simply cannot escape lockdowns. In India too, there is no other way except a lockdown. I understand it has economic consequences. But it will save lives.
Can Covid-19 vaccines be shared across countries?
We should share the intellectual property (IP) of the vaccines — anyone who used any public funding to develop these should be required to share the IP. Moving the actual vaccines from one country to another presents logistical challenges, with potential wastage due to cold storage issues, etc. We must not waste any vaccines, so sharing the IP could be the best way forward for now.
India certainly needs to intensify its vaccination program — in my view, life will return to a safe normalcy when around 80% of the population has been vaccinated. In Britain, we learnt from our previous mistakes where we had to reimpose a very damaging lockdown as a result of a hasty desire to return to normalcy. Currently, I’ve advised a very gradual easing of our lockdown because our vaccination program is not yet where it needs to be while we have an importation of a number of variants.
What would you say to those who still have vaccine hesitancy? The vaccines protect against the worst effects of Covid-19 in most people — this is extremely important. Further, all the world’s deeply committed scientists and healthcare workers are being vaccinated. There has to be a good reason for that — please follow what the experts are doing for themselves and their families.